
Children and adolescents represent a particularly vulnerable population when it comes to electromagnetic pollution (EMP). This makes it essential to thoroughly analyze the electromagnetic environments in which they live and learn—settings where exposure is increasing exponentially due to the growing number of devices they use or are surrounded by, as well as the ongoing expansion of wireless telecommunication
networks.
Several factors contribute to this heightened vulnerability among young people:
• Greater absorption of radiation. Due to their thinner skulls and higher water content in bodily tissues, children and adolescents absorb more electromagnetic energy than adults [1].
• Increased neurological sensitivity. Their nervous systems are still in development, which makes them more susceptible to potential adverse effects from EMF exposure. These effects may include impaired brain function, diminished memory and concentration, chronic fatigue, and an elevated risk of neurological disorders [2].
• Endocrine disruption. Hormonal systems in children and teens are in constant flux. Exposure to EMFs during this stage of development can interfere with hormonal regulation, potentially affecting growth, sexual maturation, and metabolic balance [3].
• Cumulative lifetime exposure. Because they are younger, children and adolescents have more years ahead of them, which increases the likelihood of experiencing long-term cumulative effects from ongoing EMF exposure.
These risks underscore the urgency of reevaluating current exposure norms and implementing stricter guidelines—particularly in environments such as homes and schools, where children and adolescents spend the majority of their time.
The Mobile Phone Problem: A Triple Harmful Interaction
The mobile phone is the primary source of artificial polarized radiation to which children and adolescents are exposed—a fact corroborated in this study. Due to its recreational and social appeal, the mobile phone has become a central element in adolescent life, to the point of being perceived as indispensable.
To fully understand the impact of mobile phones on adolescent health and well-being (and increasingly, that of children), it is essential to consider the three main dimensions through which these devices exert harm. These dimensions are interrelated and mutually reinforcing:
1. Addictive behavior and dependency. Mobile phone use is designed to create compulsive interaction. The constant stimulation from light, sound, rapid feedback, endless video content, and social rewards—such as followers, likes, and notifications—disrupts the brain’s reward systems. This effect is especially pronounced in young people, whose nervous and endocrine systems are still developing [4]. Moreover, the overstimulation linked to these devices impairs attention and concentration, which often translates into reduced reading comprehension and difficulty maintaining focus in academic settings [5].
2. Blue light exposure. Mobile screens emit high-intensity blue-violet light (400–490 nm wavelength), particularly harmful when used at night. This exposure disrupts circadian rhythms, reduces melatonin production, and contributes to sleep disorders and other biological imbalances.
3. Electromagnetic pollution. While the behavioral and lighting effects of mobile phone use have gained some public visibility, the third dimension—electromagnetic pollution—remains largely absent from mainstream discussions among policymakers and regulatory bodies. Yet this form of exposure is crucial in understanding how these three elements combine and amplify each other’s harmful effects.
For example, beyond the suppression of melatonin caused by blue light exposure, the magnetic fields emitted by mobile phones further inhibit melatonin production [2]. Compounding this, mobile phones emit both lowfrequency electromagnetic fields (from battery and internal circuitry) and high-frequency radiation (from cellular, Wi-Fi, Bluetooth, and GPS signals). Both types are biologically active and have been linked to hormonal disruption, so their combined effect is particularly concerning.
Likewise, while apps and platform design are often blamed for reducing attention spans, the underlying EMF exposure may intensify neurological symptoms such as brain fog, headaches, or difficulty concentrating [6].
In this context, the negative cognitive and emotional effects of mobile phone use cannot be attributed solely to app design, but must be understood as part of a broader, biologically mediated phenomenon. This triple harmful interaction may be one of the most detrimental influences on adolescent health today— possibly with deeper consequences than currently acknowledged by public health authorities. For this reason, future research should focus on this multifactorial impact as a pathway toward meaningful and effective
interventions.
Although the mobile phone is the most significant source of EMF exposure among adolescents, its association with socially recognized risks—such as screen addiction and blue light—may offer an opportunity for intervention. These visible issues could serve as gateways for addressing the less-recognized but equally urgent problem of electromagnetic pollution. Parents, in particular, may be more receptive to modifying their children’s usage patterns if they are made aware of the full spectrum of risks.
At the same time, it is critical to recognize that schools—where children and adolescents spend a large portion of their day—also expose them to significant and often overlooked sources of EMF. These additional exposures pose a substantial and underregulated threat to their long-term health.
Electromagnetic Pollution in Educational Settings
It is increasingly evident that educational institutions are becoming saturated with electronic devices. Computers, projectors, wireless routers, signal repeaters, and the complex electrical wiring systems required to support them have multiplied the number of sources emitting artificial, polarized electromagnetic fields (EMFs). Among the most concerning trends is the sharp rise in high-frequency emissions, which result from the demand for faster and more reliable wireless connectivity—needs that are further compounded by the widespread presence of student-owned mobile phones in classrooms.
Another growing concern is the issue of “dirty electricity”—electrical noise caused by voltage fluctuations and harmonics that result from the concurrent use of numerous electronic devices. In most schools, the electrical infrastructure was not originally designed to accommodate this level of simultaneous, high-density demand, leading to uncontrolled emissions from overloaded wiring systems.
To illustrate this problem, an in-depth environmental assessment was conducted at a secondary school in Andalusia, Spain. This institution reflects many of the characteristics common across the region: it is housed in facilities constructed in the 1970s or 1980s, an era during which much of Andalusia’s public educational infrastructure was built.
The evaluation focused on two key components necessary for a comprehensive understanding of EMF exposure:
1. A technical exploration of the physical environment, to identify electromagnetic sources and quantify exposure levels.
2. An assessment of the human factor, specifically the students who occupy the building daily and may be experiencing symptoms related to chronic EMF exposure.
This dual approach is essential for accurately characterizing the health risks associated with electromagnetic pollution in educational settings and serves as a foundation for targeted prevention strategies.
2. Methodology
This study was conducted with a sample of 72 students enrolled in various academic years, all of whom regularly attend class in the same building within a secondary education center located in the province of Granada, Spain.
To explore the relationship between symptomatology and habits related to electromagnetic hygiene, a set of two questionnaires was employed:
• EFEIA-A: This tool gathers information on students’ behaviors and habits associated with EMF exposure, including their use of mobile phones and other electronic devices, charging practices, sleeping arrangements, and duration of use.
• EFEIA-B: This version focuses on detecting physical and psychological symptoms that may be linked to exposure to electromagnetic fields. It incorporates elements adapted from international surveys designed to identify electrohypersensitivity (EHS), such as those from the Austrian Medical Association and studies conducted in Sweden.
The questionnaires were administered anonymously and completed during school hours to ensure full participation and data integrity.
In parallel, a technical inspection of the school building was performed by an engineer specializing in electromagnetic pollution. This evaluation involved the measurement of various types of electromagnetic fields—low-frequency electric and magnetic fields, high-frequency fields (radiofrequency), and dirty electricity—using calibrated, professional-grade instruments. Measurements were taken in all classrooms used by the 72 participating students, as well as in common areas such as the computer lab and music room.
By combining environmental diagnostics with self-reported data on exposure and symptomatology, this methodology enabled a comprehensive analysis of the correlation between poor electromagnetic hygiene and the presence of EHS-compatible symptoms in adolescents.
3. Results and Analysis
At the outset, 100% of participants responded “NO” when asked whether they were aware of any potential health risks associated with the use of electronic devices. Additionally, 85% reported bringing their mobile phone to school every day. This finding aligns with the data on their electromagnetic hygiene habits and suggests a general lack of awareness regarding EMF-related health implications.
Notably, 12.5% of the students (9 out of 72) achieved scores on Questionnaire B that are consistent with symptoms of electrohypersensitivity (EHS). In this instrument, a score above 110 is considered indicative of potential electrosensitivity.
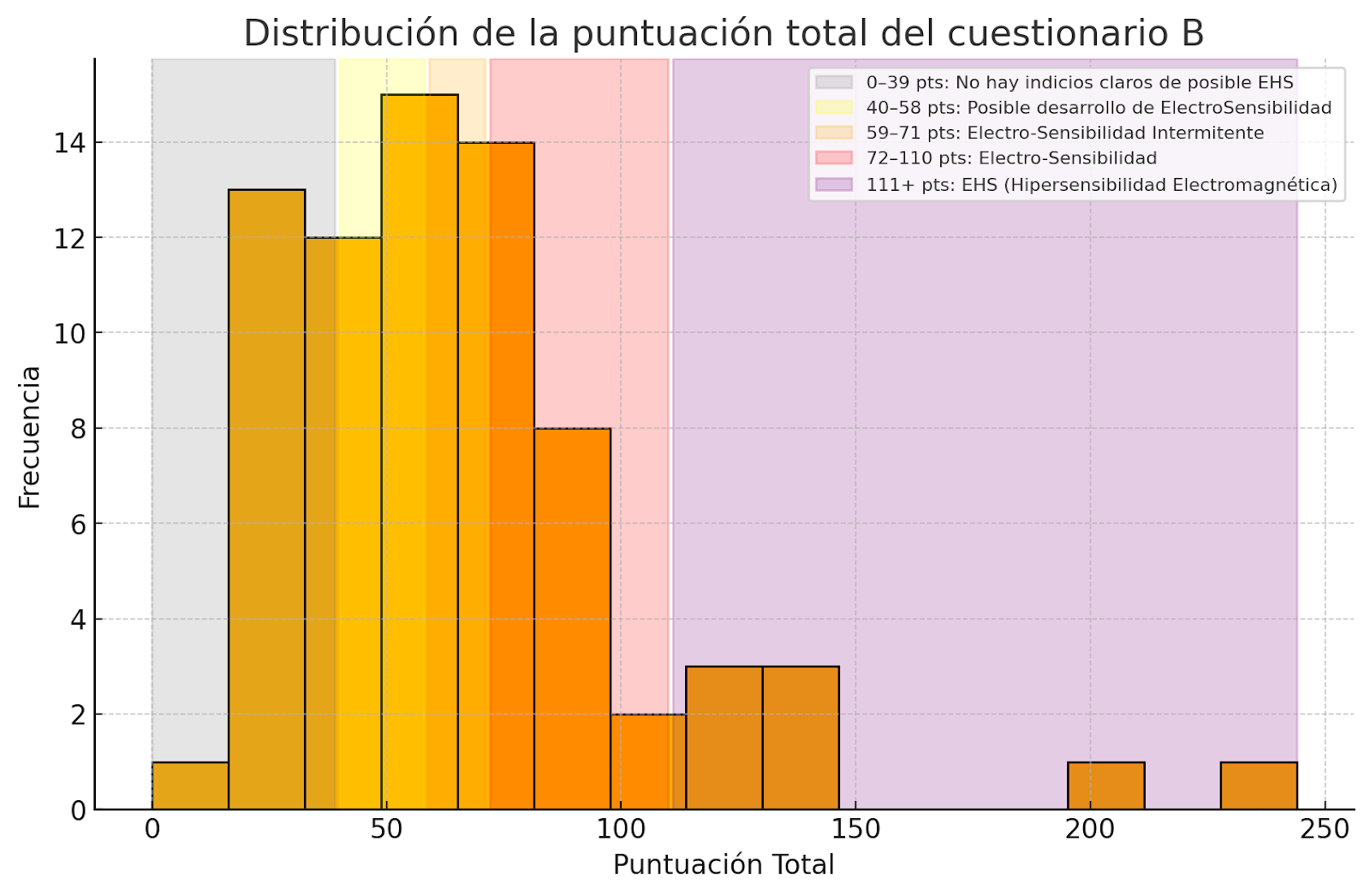
Across the entire sample, the average score was 66.64 points. The score distribution is shown in the following table, which also outlines the corresponding EHS severity level associated with each score range.
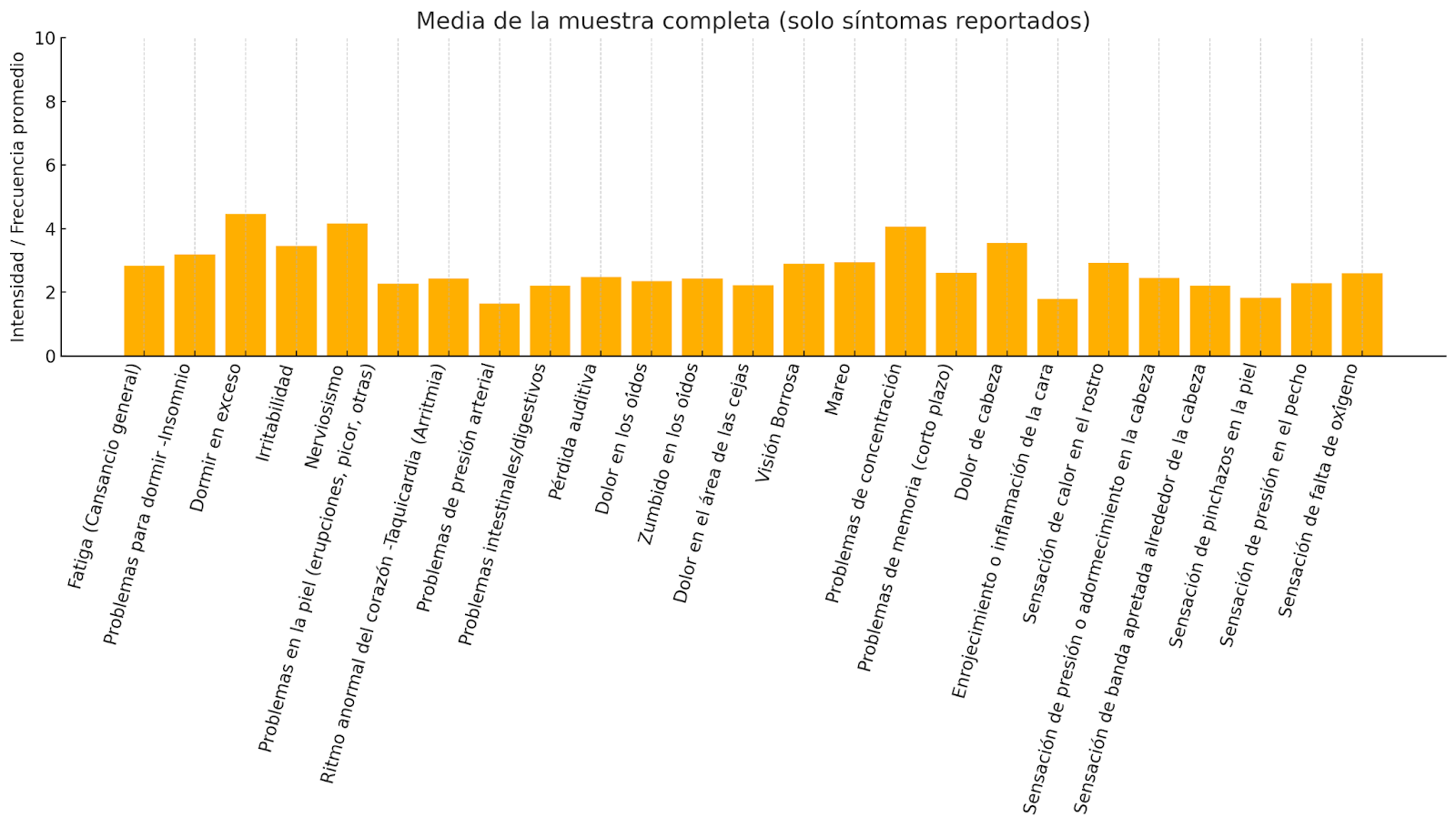
The most frequently reported symptoms—rated on a scale from 0 to 10, where 0 indicates “never” and 10 indicates “always”—were: Excessive sleepiness (mean score: 4.5), difficulty concentrating (4.1), nervousness (4.2), headaches (3.5), irritability (3.5)
As for the behavioral data collected in Questionnaire A, several notable patterns emerged:
• 22% of students reported spending more than 30 hours per week in front of electronic screens, with an overall weekly average of 22 hours.
• 38.9% indicated that they “always” or “sometimes” sleep with their phone under their pillow.
• 72.2% reported “always” or “sometimes” sleeping with their phone charging on the nightstand.
• 68% acknowledged using their phone immediately before falling asleep or even waking up during the night to check it.
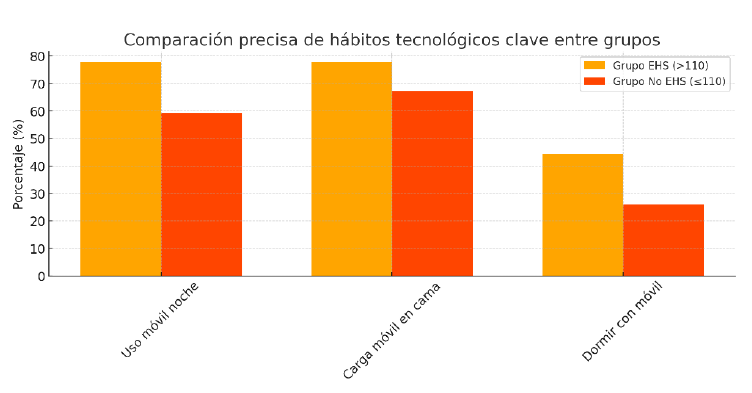
EHS group behavioral habits
Among the students who scored in the range consistent with electrohypersensitivity, harmful usage habits were significantly more pronounced. On average, these students reported using electronic devices for 36 hours per week—an increase of 66.2% compared to their non-EHS peers. Additionally, 77.8% admitted to checking their mobile phones at night in complete darkness (18.6% more than the rest of the sample), 77.8% regularly charged their phones on their nightstands while sleeping (10.6% more), and 44.4% reported sleeping with their phone under the pillow (18.4% more). These findings strongly suggest a direct correlation between poor electromagnetic hygiene and the presence of symptoms associated with electrohypersensitivity.
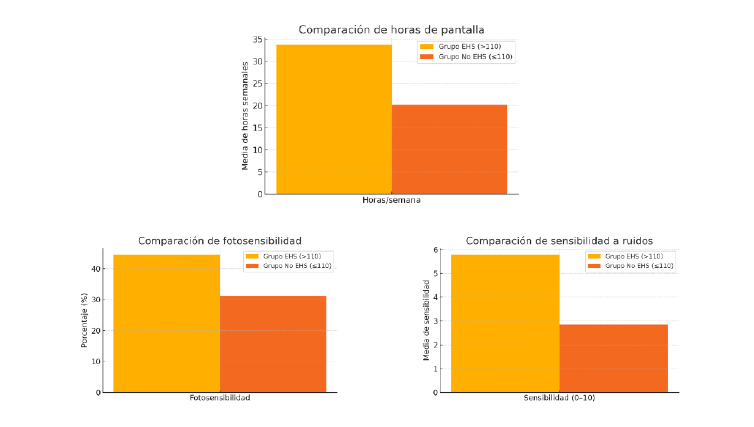
Within the overall sample, the average rate of photosensitivity was 39%. However, among students identified as potentially electrohypersensitive (EHS), this figure rose to 50%, representing an increase of 28.2%. A similar trend was observed with noise sensitivity: the average self-reported rating (on a 0–10 scale) was significantly higher in the EHS group compared to the general sample—5.78 versus 3.21, an 80% increase.
These differences support the hypothesis that increased exposure to EMF-emitting devices is associated with heightened sensory reactivity. This reactivity may be mediated by inflammatory or neurophysiological mechanisms involving the autonomic nervous system. Such findings reinforce the notion that the observed symptoms are not purely physical but also neurosensory, suggesting a possible process of progressive central sensitization.
![]()
![]()
Correlation Analysis Between Symptomatic Variables and Total Score
Based on the data collected, a Pearson correlation analysis was conducted to examine the
relationships between the quantitative variables from the questionnaire—specifically, symptomrelated variables and the participants’ total scores. The analysis revealed several notable associations, with some variables showing correlation coefficients above 0.70. These results indicate strong relationships that may carry clinical and epidemiological significance.
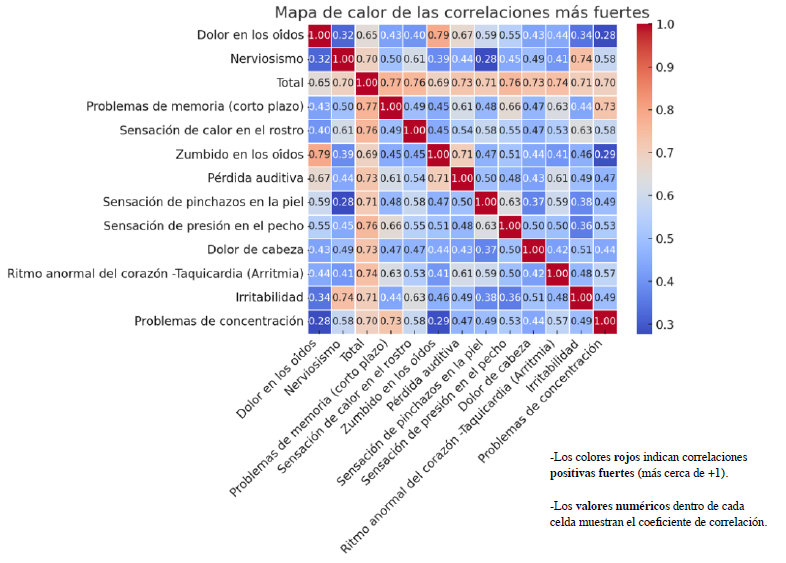
The strongest correlations were observed between the following variables:
• Ringing in the ears (tinnitus) and ear pain (r = 0.79)
• Short-term memory problems and total score (r = 0.77)
• Facial heat sensation and total score (r = 0.76)
• Tachycardia or arrhythmia and total score (r = 0.74)
• Irritability and nervousness (r = 0.74)
• Headache and total score (r = 0.73)
• Difficulty concentrating and memory problems (r = 0.73)
These findings suggest that certain cognitive symptoms (such as concentration and memory issues), auditory symptoms (such as tinnitus and ear pain), and neurophysiological symptoms (such as heart palpitations and facial heat sensations) tend to be more intense in individuals who achieved higher total scores on the questionnaire—indicating a symptom profile consistent with EHS.
The following heatmap visually represents these relationships, allowing for the identification of clusters of variables that frequently co-occur. This clustering reinforces the hypothesis that elevated total scores are influenced by the convergence of specific symptoms, and that these symptoms may be functionally interconnected or share common underlying causes.
Electromagnetic Assessment of the Common Space Occupied by the Sample
While this study does not aim to provide a comprehensive technical evaluation of the facility, it is essential to establish a reference point for the baseline level of electromagnetic pollution to which students are routinely exposed during school hours. Doing so allows us to account for a shared environmental factor across the entire sample population, thereby isolating individual, non-school exposures as a distinct variable for analysis.
Measurements were taken in the building where the surveyed students attend class. The facility consists of eight classrooms distributed across two floors. The primary sources of electromagnetic pollution include computers, projectors, Wi-Fi repeaters, sound systems, and the electrical wiring that supports these devices. Following an inspection of each classroom, the following were identified as the most significant sources of electromagnetic contamination:
1. Dirty electricity circulating through the building’s wiring showed peaks ranging from 1,600 mV to 1,920 mV. These levels are alarmingly high when compared to the maximum
recommended limit of 100 mV, or the optimal level of 33 mV established by leading
independent experts.
2. In the computer lab, constant electric fields of 100 V/m were measured on the surfaces of the desks where students work. Another classroom—specifically wired for laptop use—had electrical cables integrated into the desks, resulting in surface electric field levels of
approximately 50 V/m. These values far exceed the recommended maximum of 1.5 V/m
suggested by independent international standards for safe exposure.
3. The speakers installed in the music room emitted magnetic fields as high as 300 milligauss (mG)—well above the recommended maximum of 0.2 mG. Additionally, this room registered the highest levels of dirty electricity in the entire facility (see Figure 1). Adjacent to the music room, an exceptionally strong source of radiofrequency (RF) radiation of unknown origin was detected, with peak levels reaching 70 milliwatts per square meter (mW/m²) (see Figure 2). This is dramatically higher than the recommended safety threshold of 0.0001 mW/m².
4. Beyond this unidentified RF source, general high-frequency radiation levels throughout
the building ranged from 0.1 to 6 mW/m², depending on the classroom’s proximity to
active Wi-Fi repeaters.
Given that all students spend the same number of hours in each of the classrooms with the highest exposure levels, these measurements help us better understand the electromagnetic context in which the adolescents in this sample operate. Based on the data, it is clear that students are exposed to elevated electric fields when seated and working with computers. In contrast, magnetic field exposure tends to remain within controlled levels, generally staying below 1 milligauss (mG) in most areas—except when students are in direct physical contact with electronic devices.
In addition to environmental EMF sources, there is also considerable direct exposure stemming from the simultaneous presence of 25 to 30 active mobile phones in each classroom, one per student. This cumulative exposure represents a significant and often overlooked factor in classroom environments.
Finally, it is important to note that all lighting in the school is provided by fluorescent tubes, which produce visible flickering that can be consciously perceived. This flickering effect is known to exacerbate many of the symptoms reported in the study. Compounding the issue is the intensity of blue light within the emission spectrum of fluorescent lighting—another factor associated with visual and neurological discomfort. The problem is further aggravated by the frequent reliance on artificial lighting, as teachers often keep the window blinds closed in order to reduce glare when using projectors, thereby reducing natural light and increasing students’ exposure to artificial illumination throughout the school day.
4. Discussion
The findings of this study reveal a significant association between exposure to electromagnetic pollution (EMP) and the onset of symptoms consistent with electrohypersensitivity (EHS) in adolescents. Specifically, 12.5% of the evaluated students obtained scores indicative of potential EHS, reporting symptoms such as headaches, concentration difficulties, irritability, sleep disturbances, and daytime fatigue. This symptom profile has been previously documented in human observational studies and systematic reviews that associate these effects with exposures below the thermal limits established by organizations such as ICNIRP [9] .
One of the most relevant factors identified was the poor quality of electromagnetic hygiene among adolescents with symptoms, particularly regarding nighttime mobile phone use. Among students reporting EHS-compatible symptoms, 77.8% used their phones in bed in complete darkness—or even woke up during the night to use them—and 44.4% slept with their phones under their pillows.
These habits involve sustained exposure to extremely low frequencies (ELF) and radiofrequency (RF) radiation during a critical phase of the circadian cycle, with potential consequences for melatonin secretion. The suppression of melatonin induced by electromagnetic exposure has been extensively documented in experimental and clinical studies, which have also shown notable improvements in sleep following the reduction of low-frequency magnetic field exposure [9] .
Additionally, this subgroup exhibited a high prevalence of photosensitivity (50%) and auditory sensitivity (mean score of 5.78 out of 10), which may be linked to dysfunctions of the autonomic nervous system triggered by electromagnetic exposure. This connection has been described by Lai in his reviews on the neurological effects of radiofrequencies, and by Grigoriev and Khorseva in a longitudinal study (2006–2017) involving Russian schoolchildren, which found neuropsychological changes associated with frequent mobile phone use [10] .
The correlation analyses based on the questionnaire results revealed consistent patterns in the cooccurrence of symptoms related to electronic device exposure, reinforcing the hypothesis of an organized syndrome rather than a random array of complaints. Pearson’s correlation allowed for the examination of linear relationships between various quantified variables, revealing strong associations among numerous physical, cognitive, and autonomic symptoms.
Specifically, high correlations were observed between auditory symptoms such as tinnitus and ear pain (r = 0.79), suggesting a possible shared pathophysiological mechanism. Likewise, cognitive symptoms—such as memory and concentration difficulties—were strongly interrelated and correlated with the total symptom score (r = 0.77 and r = 0.73, respectively), indicating that cognitive impairment may be a central feature of the reported clinical picture.
Significant associations were also found between the total score and autonomic symptoms such as tachycardia (r = 0.74), headaches (r = 0.73), and facial heat sensation (r = 0.76). These associations may reflect dysfunctions in the autonomic nervous system, a finding previously suggested in studies on individuals with electromagnetic sensitivity.
A heatmap generated from the strongest correlations helped visualize these relationships, showing well-defined clusters of symptoms that tend to occur together. This internal structure reinforces the idea that the syndrome described by high-scoring individuals exhibits internal consistency, and that symptoms do not occur in isolation, but rather as part of an interrelated and potentially cumulative process.
From an epidemiological perspective, the severity of symptoms observed in such a young
population is striking—especially considering the cumulative nature of long-term exposure to electromagnetic fields. The presence of strong correlations among the most frequently reported symptoms provides quantitative evidence supporting the internal validity of the assessment tool used, and underscores the need for future longitudinal research to assess causality.
Regarding the physical environment, the levels of dirty electricity detected within the school building far exceeded the reference values proposed by independent organizations. This form of electrical pollution—consisting of high-frequency harmonics superimposed on the alternating current—has been implicated in both physiological and immune dysfunctions, as demonstrated in the study by Maisch et al. involving chronic fatigue patients [10] and in additional research linking dirty electricity to behavioral issues and attention deficits [11] .
Despite the strength of these findings, the study has evident limitations. The sample size is
relatively modest (n = 72), and the lack of an unexposed external control group limits the
generalizability of the results. Nevertheless, the ability to analyze two distinct subgroups within the sample—EHS and non-EHS—under conditions of complete environmental homogeneity during school hours, along with the rural setting and the relatively balanced distribution of local electromagnetic sources, enhances the reliability of the selected sample. Furthermore, the internal consistency observed between reported symptoms and exposure-related habits indicates a pattern that aligns with existing scientific literature on electrohypersensitivity, as emphasized in the critical reviews conducted by the ICBE-EMF commission [12].
Finally, it is considered essential to expand upon this research through longitudinal studies that evaluate changes in symptomatology following improvements in electromagnetic hygiene. It is also recommended to incorporate objective physiological biomarkers—such as melatonin and cortisol levels, or heart rate variability analysis—to strengthen the evidence for causality and support the development of clinical protocols for the diagnosis and treatment of electrohypersensitivity in adolescents [11].
5. Final Conclusions and Recommendations
After analyzing both the habits and symptomatology of the student population, and assessing the physical space of the school in which they spend six and a half hours daily, the following conclusions can be drawn:
1. The mobile phone is the primary source of electromagnetic pollution to which students
are exposed. As previously discussed, this exposure is further intensified by a triple harmful
interaction that occurs for many hours during direct contact with the device.
2. There is a direct correlation between poor electromagnetic exposure habits, symptomatology consistent with electrohypersensitivity, and sensory hyperreactivity— indicative of a central sensitization process—when compared to the average values of the non-EHS group.
3. While the exact impact of electromagnetic pollution in the school setting on students cannot be precisely determined, the level of dirty electricity detected is nearly 20 times higher than the 100 mV maximum recommended by reference organizations [7] . Dirty electricity is the primary emitter of EM pollution in this environment due to its industrial-level values. This highlights a key issue in educational centers: the ongoing expansion and increasing use of electronic devices is not matched by adaptations or improvements to the building's electrical infrastructure. This neglect is further reflected in the fact that most power outlets have reversed phase and neutral wiring. Although RF exposure is not excessive in relative terms, considering the hyperconnected world we live in, it reaches levels up to 60,000 times higher than recommended reference values [8].
4. In addition to mobile phone usage, the high levels of dirty electricity and RF radiation
recorded—as well as the constant exposure to them—could be among the causal factors behind the high rate of electrohypersensitivity (12.5%) observed in this study. This figure is considerably higher than the estimated 5% prevalence in highly polluted urban populations [13] .
5. The lack of natural lighting in the school, along with the use of fluorescent tubes, may
exacerbate the symptoms experienced by students and contribute to the high average level of photosensitivity observed in the sample.
Given the circumstances described above, the following recommendations are proposed:
• A comprehensive technical study should be conducted within the school to significantly
reduce students' exposure to electromagnetic pollution. This would include an assessment and update of the electrical installation to meet current demands of electronic equipment, relocation of certain devices if necessary, and the implementation of passive filtering systems to eliminate EM pollution generated by both wireless and hardwired devices. This plan should also explore upgrading the lighting system, replacing fluorescent tubes with alternatives that reduce dirty electricity and offer a more favorable light spectrum.
• The widespread lack of awareness regarding the risks of electromagnetic pollution—
evident from the fact that nearly all students carry their phones in their pockets and the poor EM hygiene reflected in questionnaire responses—demonstrates the urgent need for an educational and awareness program focused on EM pollution and its potential health
effects. This program should operate at three levels: targeting parents, teachers (including
school leadership), and students, with content tailored to each group’s level of awareness
and capacity. A specialized workshop on electromagnetic hygiene should be designed
specifically for students.
Given the difficulty of implementing such a program in a single public school and the limited impact it would have if done in isolation, it is recommended that this initiative be centralized and rolled out across the entire Andalusian public school network, coordinated by the Regional Ministry of Education.